
READ PDF REPLY: Lennart Hardell, MD, PhD-SCENIHR 2013 comments
European Commission
Health & Consumers
Directorate C: Public Health
Unit C2 – Health Information/ Secretariat of the Scientific Committee
Office: HTC 03/073 L-2920 Luxembourg
SANCO-‐C2-‐
Comments on the RF fields epidemiology section pages 57-68 in SCENIHR approved at the 4th plenary of 12 December 2013
We have read the SCENIHR 2013 Preliminary opinion on Potential health effects of exposure to electromagnetic fields (EMF), especially relating to epidemiological studies on neoplastic diseases. It is concluded at page 4 in the abstract that “Based on the most recent cohort and incidence time trend studies, it appears that the evidence for glioma became weaker while the possibility of an association with acoustic neuroma remains open”.
This statement is not based on facts but on selective inclusion of studies with omission of the most recent publications, e.g. from our research group (the Hardell group). Our studies were well known to the Expert group since Dr Kjell Hansson Mild was one of these experts and also a co-author in most of the Hardell group studies. In fact he communicated our studies to the SCENIHR expert group obviously without response. If these studies had been included it would be apparent that the final conclusions on brain tumour risk in SCENIHR are not based on scientific facts. In contrast the evidence for glioma and acoustic neuroma would become stronger if recent publications had been included.
In the Terms of Reference (page 16) it is stated that the Committee is requested e.g.:
- To update its opinions of 2009 in the light of newly available information
- To give particular attention to issues affected by important gaps in knowledge in the previous opinions, especially:
- The potential adverse effects of EMF on the nervous system, including neurobehavioral disorders, and on the risk of neo-plastic diseases; It seems as if the Committee has been anxious to include ‘newly available information’ at least regarding some studies, e.g. Benson VS, Pirie K, Schüz J, Reeves GK, Beral V, Green J. Int J Epidemiol 2013, Sep 27, see page 64, not included in reference list. On the contrary our studies were excluded. In the following a summary is given.
Background:
The carcinogenic effect of RF-EMF on humans was evaluated at a meeting during 24 – 31 May 2011 at the International Agency for Research on Cancer (IARC) at WHO in Lyon,
France. The Working Group consisted of 30 scientists representing four areas: ‘animal cancer studies’, ‘epidemiology’, ‘exposure’ and ‘mechanistic and other relevant data’
(http://monographs.iarc.fr/ENG/Meetings/vol102-participants.pdf). One of us, LH, was invited as an expert in the epidemiology group. On 31 May 2011 IARC categorised RF-EMFs
from mobile phones, and from other devices that emit similar non-ionising electromagnetic fields, as a Group 2B, i.e. a ‘possible’, human carcinogen. The decision was almost unanimous. No consistent evidence was found for meningioma, a benign type of brain tumour. After the IARC meeting we have published further studies with new data, both overview of studies with meta-analysis (number 1 below) and our case-control study including brain tumour cases diagnosed during 2007-2009 (number 2-4 below). Furthermore we applied the Hill viewpoints on the risk for brain tumours associated with use of mobile and cordless phones (number 5 below). These criteria were developed in the 1960’s during the height of the tobacco and lung cancer controversy.
Recent studies from the Hardell group not included in SCENIHR 2013:
1. Hardell L, Carlberg M, Hansson Mild K. Use of mobile phones and cordless phones is associated with increased risk for glioma and acoustic neuroma. Pathophysiology 2013;20:85-110. Epub 2012 Dec 21.
Abstract
The International Agency for Research on Cancer (IARC) at WHO evaluation of the carcinogenic effect of RF-EMF on humans took place during a 24-31 May 2011 meeting at Lyon in France. The Working Group consisted of 30 scientists and categorised the radiofrequency electromagnetic fields from mobile phones, and from other devices that emit similar non-ionising electromagnetic fields (RF-EMF), as Group 2B, i.e., a ‘possible’, human carcinogen. The decision on mobile phones was based mainly on the Hardell group of studies from Sweden and the IARC Interphone study. We give an overview of current epidemiological evidence for an increased risk for brain tumours including a meta-analysis of the Hardell group and Interphone results for mobile phone use. Results for cordless phones are lacking in Interphone. The meta-analysis gave for glioma in the most exposed part of the brain, the temporal lobe, odds ratio (OR)=1.71, 95% confidence interval (CI)=1.04-2.81 in the ≥10 years (>10 years in the Hardell group) latency group. Ipsilateral mobile phone use ≥1640h in total gave OR=2.29, 95% CI=1.56-3.37. The results for meningioma were OR=1.25, 95% CI=0.31-4.98 and OR=1.35, 95% CI=0.81-2.23, respectively. Regarding acoustic neuroma ipsilateral mobile phone use in the latency group ≥10 years gave OR=1.81, 95% CI=0.73-4.45. For ipsilateral cumulative use ≥1640h OR=2.55, 95% CI=1.50-4.40 was obtained. Also use of cordless phones increased the risk for glioma and acoustic neuroma in the Hardell group studies. Survival of patients with glioma was analysed in the Hardell group studies yielding in the >10 years latency period hazard ratio (HR)=1.2, 95% CI=1.002-1.5 for use of wireless phones. This increased HR was based on results for astrocytoma WHO grade IV (glioblastoma multiforme). Decreased HR was found for low-grade astrocytoma, WHO grades I-II, which might be caused by RF-EMF exposure leading to tumour-associated symptoms and earlier detection and surgery with better prognosis. Some studies show increasing incidence of brain tumours whereas other studies do not. It is concluded that one should be careful using incidence data to dismiss results in analytical epidemiology. The IARC carcinogenic classification does not seem to have had any significant impact on governments’ perceptions of their responsibilities to protect public health from this widespread source of radiation.
2. Carlberg M, Söderqvist F, Hansson Mild K, Hardell L. Meningioma patients diagnosed 2007-2009 and the association with use of mobile and cordless phones, Environ. Health 2013;12:60, doi:10.1186/1476-069X-12-60. Epub Jul 19, 2013
Abstract
BACKGROUND: To study the association between use of wireless phones and meningioma. METHODS: We performed a case–control study on brain tumour cases of both genders aged 18–75 years and diagnosed during 2007–2009. One population-based control matched on gender and age was used to each case. Here we report on meningioma cases including all available controls. Exposures were assessed by a questionnaire. Unconditional logistic regression analysis was performed.
RESULTS: In total 709 meningioma cases and 1,368 control subjects answered the questionnaire. Mobile phone use in total produced odds ratio (OR) = 1.0, 95% confidence interval (CI) = 0.7-1.4 and cordless phone use gave OR = 1.1, 95% CI = 0.8-1.5. The risk increased statistically significant per 100 h of cumulative use and highest OR was found in the fourth quartile (>2,376 hours) of cumulative use for all studied phone types. There was no statistically significant increased risk for ipsilateral mobile or cordless phone use, for meningioma in the temporal lobe or per year of latency. Tumour volume was not related to latency or cumulative use in hours of wireless phones.
CONCLUSIONS: No conclusive evidence of an association between use of mobile and cordless phones and meningioma was found. An indication of increased risk was seen in the
group with highest cumulative use but was not supported by statistically significant increasing risk with latency. Results for even longer latency periods of wireless phone use than in this
study are desirable.
3. Hardell L. Carlberg M, Söderqvist F, Hansson Mild K. Pooled analysis of case-control studies on acoustic neuroma diagnosed 1997-2003 and 2007-2009 and use of mobile and cordless phones. Int J Oncol. 2013;43:1036-1044. Epub 2013 Jul 22.
Abstract
We previously conducted a case-control study of acoustic neuroma. Subjects of both genders aged 20-80 years, diagnosed during 1997-2003 in parts of Sweden, were included, and the results were published. We have since made a further study for the time period 2007-2009 including both men and women aged 18-75 years selected from throughout the country. These new results for acoustic neuroma have not been published to date. Similar methods were used for both study periods. In each, one population-based control, matched on gender and age (within five years), was identified from the Swedish Population Registry. Exposures were assessed by a self-administered questionnaire supplemented by a phone interview. Since the number of acoustic neuroma cases in the new study was low we now present pooled results from both study periods based on 316 participating cases and 3,530 controls. Unconditional logistic regression analysis was performed, adjusting for age, gender, year of diagnosis and socio-economic index (SEI). Use of mobile phones of the analogue type gave odds ratio (OR) = 2.9, 95% confidence interval (CI) = 2.0-4.3, increasing with >20 years latency (time since first exposure) to OR = 7.7, 95% CI = 2.8-21. Digital 2G mobile phone use gave OR = 1.5, 95% CI = 1.1-2.1, increasing with latency >15 years to an OR = 1.8, 95% CI = 0.8-4.2. The results for cordless phone use were OR = 1.5, 95% CI = 1.1-2.1, and, for latency of >20 years, OR = 6.5, 95% CI = 1.7-26. Digital type wireless phones (2G and 3G mobile phones and cordless phones) gave OR = 1.5, 95% CI = 1.1-2.0 increasing to OR = 8.1, 95% CI = 2.0-32 with latency >20 years. For total wireless phone use, the highest risk was calculated for the longest latency time >20 years: OR = 4.4, 95% CI = 2.2-9.0. Several of the calculations in the long latency category were based on low numbers of exposed cases. Ipsilateral use resulted in a higher risk than contralateral for both mobile and cordless phones. OR increased per 100 h cumulative use and per year of latency for mobile phones and cordless phones, though the increase was not statistically significant for cordless phones. The percentage tumour volume increased per year of latency and per 100 h of cumulative use, statistically significant for analogue phones. This study confirmed previous results demonstrating an association between mobile and cordless phone use and acoustic neuroma.
4. Hardell L, Carlberg M, Söderqvist F, Hansson Mild K. Case-control study of the association between malignant brain tumors diagnosed 2007-2009 and mobile and cordless phone use. Int J Oncol. 2013;43:1833-1845. Epub 2013 Sep 24
Abstract
Previous studies have shown a consistent association between long-term use of mobile and cordless phones and glioma and acoustic neuroma, but not for meningioma. When used these phones emit radiofrequency electromagnetic fields (RF-EMFs) and the brain is the main target organ for the handheld phone. The International Agency for Research on Cancer (IARC) classified in May, 2011 RF-EMF as a group 2B, i.e. a ‘possible’ human carcinogen. The aim of this study was to further explore the relationship between especially long-term (>10 years) use of wireless phones and the development of malignant brain tumours. We conducted a new case-control study of brain tumour cases of both genders aged 18-75 years and diagnosed during 2007-2009. One population-based control matched on gender and age (within 5 years) was used to each case. Here, we report on malignant cases including all available controls. Exposures on e.g. use of mobile phones and cordless phones were assessed by a self-administered questionnaire. Unconditional logistic regression analysis was performed, adjusting for age, gender, year of diagnosis and socio-economic index using the whole control sample. Of the cases with a malignant brain tumour, 87% (n=593) participated, and 85% (n=1,368) of controls in the whole study answered the questionnaire. The odds ratio (OR) for mobile phone use of the analogue type was 1.8, 95% confidence interval (CI)=1.04-3.3, increasing with >25 years of latency (time since first exposure) to an OR=3.3, 95% CI=1.6-6.9. Digital 2G mobile phone use rendered an OR=1.6, 95% CI=0.996-2.7, increasing with latency >15-20 years to an OR=2.1, 95% CI=1.2-3.6. The results for cordless phone use were OR=1.7, 95% CI=1.1-2.9, and, for latency of 15-20 years, the OR=2.1, 95% CI=1.2-3.8. Few participants had used a cordless phone for >20-25 years. Digital type of wireless phones (2G and 3G mobile phones, cordless phones) gave increased risk with latency >1-5 years, then a lower risk in the following latency groups, but again increasing risk with latency >15-20 years. Ipsilateral use resulted in a higher risk than contralateral mobile and cordless phone use. Higher ORs were calculated for tumours in the temporal and overlapping lobes. Using the meningioma cases in the same study as reference entity gave somewhat higher ORs indicating that the results were unlikely to be explained by recall or observational bias. This study confirmed previous results of an association between mobile and cordless phone use and malignant brain tumours. These findings provide support for the hypothesis that RF-EMFs play a role both in the initiation and promotion stages of carcinogenesis.
5. Hardell L, Carlberg M. Using the Hill viewpoints from 1965 for evaluating strengths of evidence of the risk for brain tumors associated with use of mobile and cordless phones. Rev Environ Health 2013;38:97-106. doi: 10.1515/reveh-2013-0006.
Abstract
BACKGROUND: Wireless phones, i.e., mobile phones and cordless phones, emit radiofrequency electromagnetic fields (RF-EMF) when used. An increased risk of brain tumors is a major concern. The International Agency for Research on Cancer (IARC) at the World Health Organization (WHO) evaluated the carcinogenic effect to humans from RFEMF in May 2011. It was concluded that RF-EMF is a group 2B, i.e., a “possible”, human carcinogen. Bradford Hill gave a presidential address at the British Royal Society of Medicine in 1965 on the association or causation that provides a helpful framework for evaluation of the brain tumor risk from RF-EMF.
METHODS: All nine issues on causation according to Hill were evaluated. Regarding wireless phones, only studies with long-term use were included. In addition, laboratory studies and data on the incidence of brain tumors were considered.
RESULTS: The criteria on strength, consistency, specificity, temporality, and biologic gradient for evidence of increased risk for glioma and acoustic neuroma were fulfilled. Additional evidence came from plausibility and analogy based on laboratory studies.
Regarding coherence, several studies show increasing incidence of brain tumors, especially in the most exposed area. Support for the experiment came from antioxidants that can alleviate the generation of reactive oxygen species involved in biologic effects, although a direct mechanism for brain tumor carcinogenesis has not been shown. In addition, the finding of no increased risk for brain tumors in subjects using the mobile phone only in a car with an external antenna is supportive evidence. Hill did not consider all the needed nine viewpoints to be essential requirements.
CONCLUSION: Based on the Hill criteria, glioma and acoustic neuroma should be considered to be caused by RF-EMF emissions from wireless phones and regarded as carcinogenic to humans, classifying it as group 1 according to the IARC classification. Current guidelines for exposure need to be urgently revised.
Summary
During 2013 our research group has published results from further studies on brain tumour risk associated with use of mobile and/or cordless desktop phones. We published data on tumour risk for use of these devices during 20 years or more. Clearly we find again an increased risk for malignant brain tumours including the most common type glioma (‘brain cancer’). We find also increased risk of acoustic neuroma, a benign tumour of the hearing nerve (number VIII). These tumours usually lead to hearing problems (deafness), tinnitus and dizziness although rarely lethal. Still we find no clear increased risk for meningioma, even after 20 years use of the mobile phone.
Especially worrying is that we find highest risk for glioma and acoustic neuroma in subjects who started use of the wireless phone before the age of 20 years. We have also found that the prognosis of glioma (astrocytoma grade IV) is worse the longer time one has used the wireless phone. That means that long-term use shortens the survival.
Further research has thus strengthened the evidence in support of an increased risk of malignant brain tumours and acoustic neuroma associated with use of mobile phones. Based on the latest findings and using the so called Hill viewpoints from the 1960’s exposure to RF6 EMF from mobile phones may now be classified as a human cancer causing agent, Group 1, according to the definitions used by IARC.
It is unfortunate that SCENIHR has disregarded these findings and instead relies heavily on the much criticised Danish cohort study on mobile phone users with poor exposure data. We have discussed the many shortcomings in that study, see Söderqvist F, Carlberg M, Hardell L. Review of four publications on the Danish cohort study on mobile phone subscribers and risk of brain tumors. Reviews Environmental Health. 2012; 27: 51-58. SCENIHR lacks reference to our publication and accordingly also critical comments on the Danish cohort study. The same lack of critical review applies to the study by Benson et al, included in SCENIHR, but without acknowledge of the limitations in that study.
The CEFALO study on brain tumour risk in children is included in SCENIHR, however without a critical review of the study. For example use of cordless phones was assessed only during the 3 first years of use, a most peculiar definition. Our review of that study is omitted from SCENIHR, see Söderqvist F, Carlberg M, Hansson Mild K, Hardell L. Childhood brain tumour risk and its association with wireless phones: a commentary. Environmental Health. 2011; 10: 106.
In addition to the Danish cohort study and the UK study by Benson et al SCENIHR relies heavily on time trend analyses. However the conclusion by IARC in the 2011 evaluation was that: “Time-trend analyses did not show an increased rate of brain tumours after the increase in mobile phone use. However, these studies have substantial limitations because most of the analyses examined trends until the early 2000s only. Such analyses are uninformative if excess risk only manifests more than a decade after phone use begins, or if phone use only affects a small proportion of cases—eg, the most heavily exposed, or a subset of brain tumours.” See Baan R, Grosse Y, Lauby-Secretan B, et al. Carcinogenicity of radiofrequency electromagnetic fields. Lancet Oncology. 2011; 12: 624-626.
In our publication number 4 above, we presented restricted cubic spline plot of the relationship between latency of wireless phone use and malignant brain tumours, see figure below. The solid line indicates the OR estimate and the broken lines represent the 95% CI. Adjustment was made for age at diagnosis, gender, SEI-code and year of diagnosis. Obviously the latency is 20+ years for malignant brain tumours according to these results. Thus, it confirms the conclusion by IARC on incidence data that “Such analyses are uninformative if excess risk only manifests more than a decade after phone use begins”; in fact it may even be two decades based on our data. Our results are also in agreement with de Vocht et al “According to these ecological results the latency period is at least 11-12 years, but probably more than 20 years.” See de Vocht F, Hannam K, Buchan I. Environmental risk factors for cancers of the brain and nervous system: the use of ecological data to generate hypotheses. Occup Environ Med 2013; 70: 349-356.
In summary, the preliminary SCENIHR conclusion that glioma risk is weaker now is not scientifically justified. The only way that conclusion could be reached by SCENIHR is to exclude critical studies that present evidence to the contrary, i.e. studies that report the risk of glioma (and acoustic neuroma) is stronger now than in 2009. Including our studies would give different conclusions supported by critical review of the limitations in cohort studies and incidence data. The Preliminary Opinion should be sent back to the Committee for new evaluation of the scientific data, and should integrate the results of these published data.
1) Hardell L, Carlberg M, Hansson Mild K. Use of mobile phones and cordless phones is associated with increased risk for glioma and acoustic neuroma. Pathophysiology 2013;20:85-110. Epub 2012 Dec 21.
2. Carlberg M, Söderqvist F, Hansson Mild K, Hardell L. Meningioma patients diagnosed 2007-2009 and the association with use of mobile and cordless phones, Environ. Health 2013;12:60, doi:10.1186/1476-069X-12-60.
Epub Jul 19, 2013
3. Hardell L. Carlberg M, Söderqvist F, Hansson Mild K. Pooled analysis of case-control studies on acoustic neuroma diagnosed 1997-2003 and 2007-2009 and use of mobile and cordless phones. Int J Oncol. 2013;43:1036-1044. Epub 2013 Jul 22.
4. Hardell L, Carlberg M, Söderqvist F, Hansson Mild K. Case-control study of the association between malignant brain tumors diagnosed 2007-2009 and mobile and cordless phone use. Int J Oncol. 2013;43:1833-1845. Epub 2013 Sep 24
5. Hardell L, Carlberg M. Using the Hill viewpoints from 1965 for evaluating strengths of evidence of the risk for brain tumors associated with use of mobile and cordless phones. Rev Environ Health 2013;38:97-106. doi:10.1515/reveh-2013-0006.
Respectfully submitted
Lennart Hardell, MD, PhD
Professor
Department of Oncology
University Hospital
SE-701 85 Örebro
Sweden
Fredrik Söderqvist, PhD
Epidemiologist
Department of Public Health and Community Medicine & Centre of Clinical Research
County Council of Vestmanland & Uppsala University
70289 Västerås
Sweden
Michael Carlberg, MSc
Department of Oncology
University Hospital
SE-701 85 Örebro
Sweden
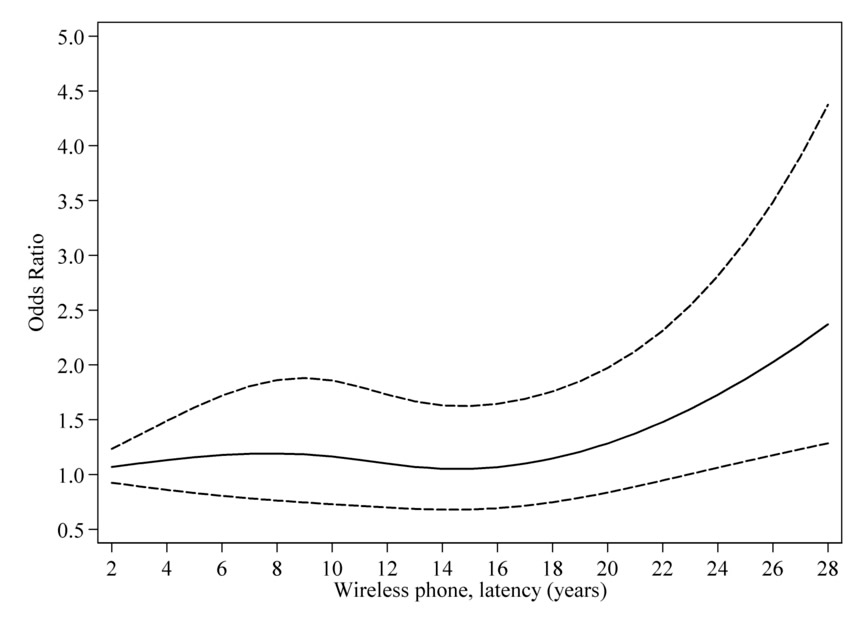
Restricted cubic spline plot of the relationship between latency of wireless phones and malignant brain tumours. The solid line indicates the OR estimate and the broken lines represent the 95% CI. Adjustment was made for age at diagnosis, gender, SEI-code and year of diagnosis. Population based controls were used. (Hardell et al Int J Oncol. 013;43:1833-1845.
Epub 2013 Sep 24)